


 Sign Out
Sign Out




Pharmacology: Pharmacodynamics: Tiotropium bromide is a long-acting, specific antagonist at muscarinic receptors. It has similar affinity to the subtypes, M1 to M5. In the airways, tiotropium bromide competitively and reversibly binds to the M3 receptors in the bronchial smooth musculature, antagonising the cholinergic (bronchoconstrictive) effects of acetylcholine, resulting in bronchial smooth muscle relaxation. The effect was dose dependent and lasted longer than 24 h. As an N-quaternary anticholinergic, tiotropium bromide is topically (broncho-) selective when administered by inhalation, demonstrating an acceptable therapeutic range before systemic anticholinergic effects may occur.
The dissociation of tiotropium from especially M3-receptors is very slow, exhibiting a significantly longer dissociation half-life than ipratropium. Dissociation from M2-receptors is faster than from M3, which in functional in vitro studies, elicited (kinetically controlled) receptor subtype selectivity of M3 over M2. The high potency, very slow receptor dissociation and topical inhaled selectivity found its clinical correlate in significant and long-acting bronchodilation in patients with COPD and asthma.
COPD: The clinical Phase III development programme for COPD included two 1-year, two 12-weeks and two 4-weeks randomised, double-blind studies in 2901 COPD patients (1038 receiving the 5 μg tiotropium dose). The 1-year programme consisted of two placebo-controlled trials. The two 12-week trials were both active (ipratropium)- and placebo-controlled. All six studies included lung function measurements. In addition, the two 1-year studies included health outcome measures of dyspnoea, health-related quality of life and effect on exacerbations.
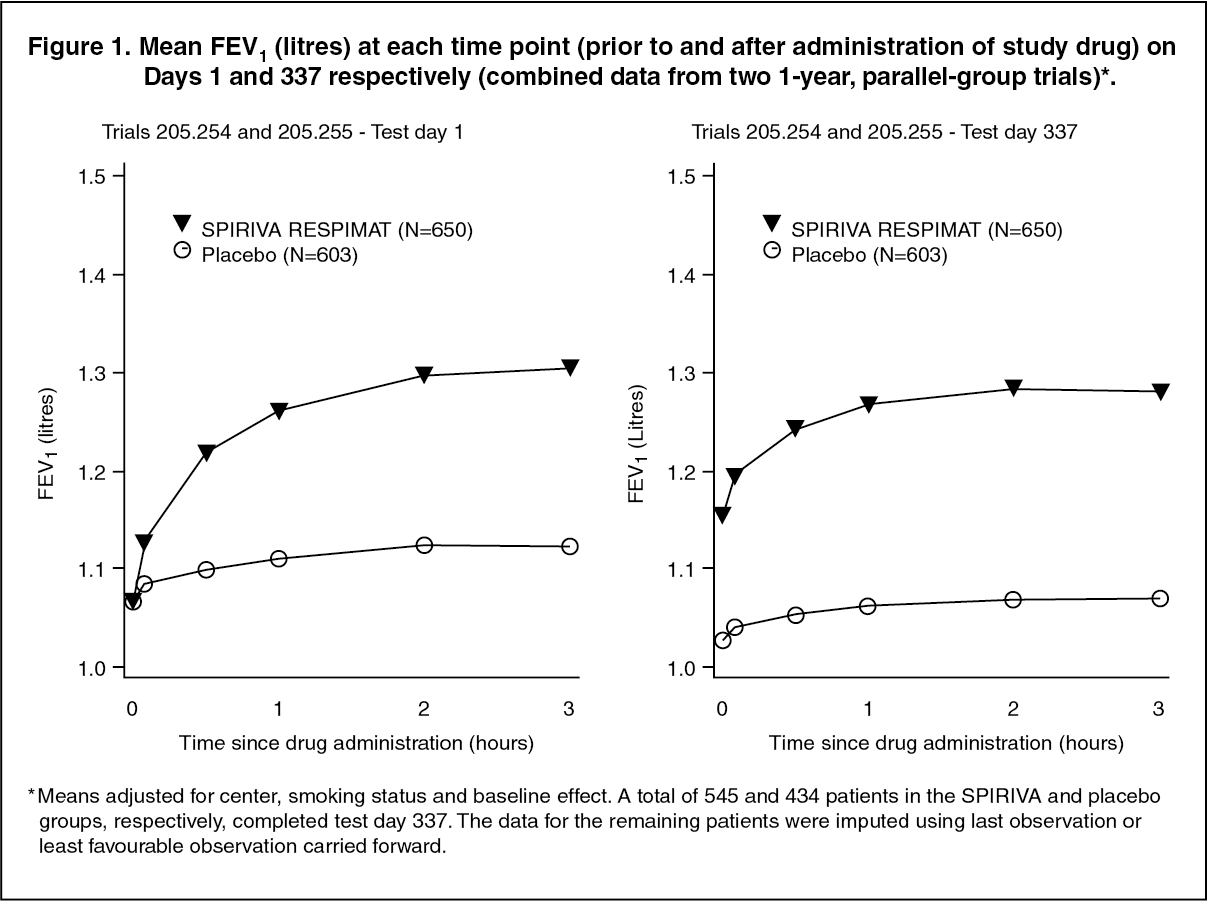
Placebo-controlled studies: Lung function: SPIRIVA RESPIMAT, administered once daily, provided significant improvement in lung function (forced expiratory volume in one second and forced vital capacity) within 30 minutes following the first dose, compared to placebo (FEV1 mean improvement at 30 minutes: 0.113 litres; 95% confidence interval (CI): 0.102 to 0.125 litres, p< 0.0001). Improvement of lung function was maintained for 24 hours at steady state compared to placebo (FEV1 mean improvement: 0.122 litres; 95% CI: 0.106 to 0.138 litres, p< 0.0001).
Pharmacodynamic steady state was reached within one week.
Spiriva Respimat significantly improved morning and evening PEFR (peak expiratory flow rate) as measured by patient's daily recordings compared to placebo (PEFR mean improvement: mean improvement in the morning 22 L/min; 95% CI: 18 to 55 L/min, p< 0.0001; evening 26 L/min; 95% CI: 23 to 30 L/min, p<0.0001). The use of Spiriva Respimat resulted in a reduction of rescue bronchodilator use compared to placebo (mean reduction in rescue use 0.66 occasions per day, 95% CI: 0.51 to 0.81 occasions per day, p<0.0001).
The bronchodilator effects of Spiriva Respimat were maintained throughout the 1-year period of administration with no evidence of tolerance. (See Figures 1, 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image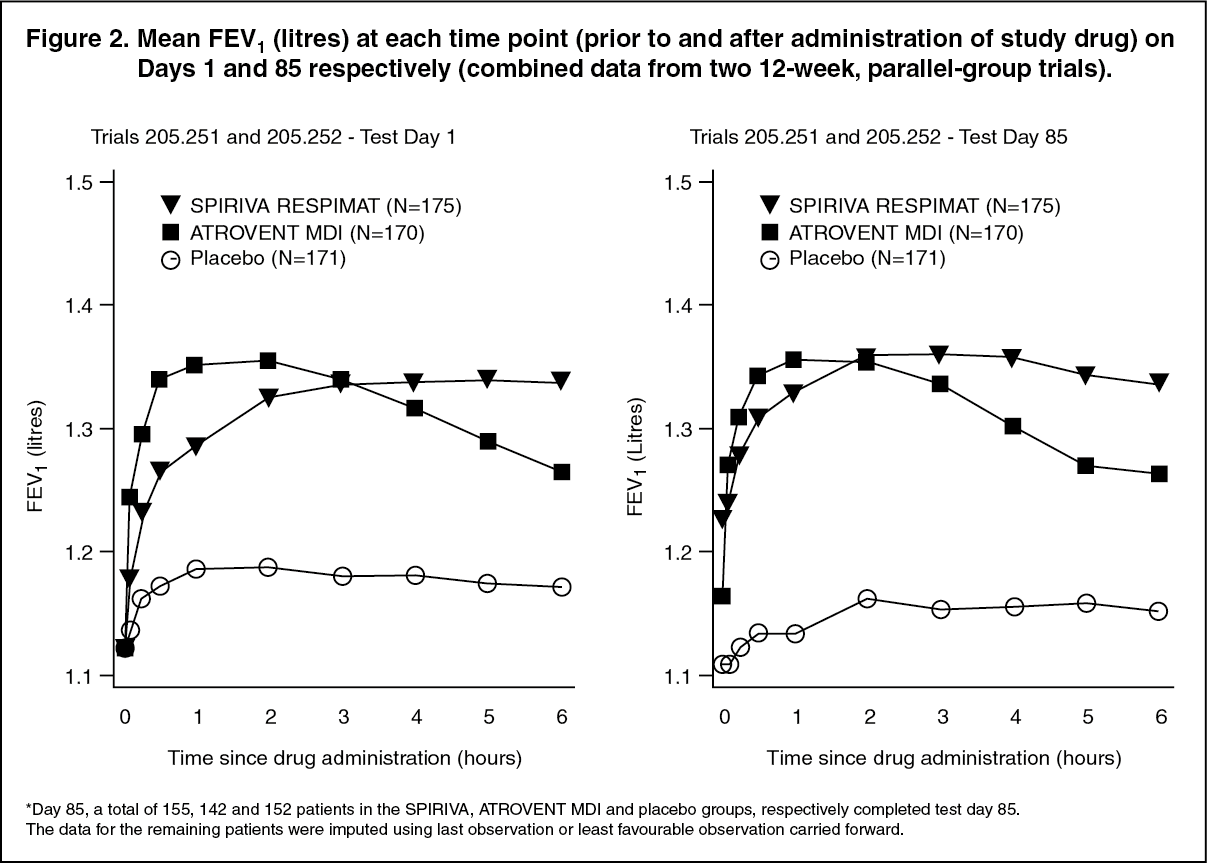 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image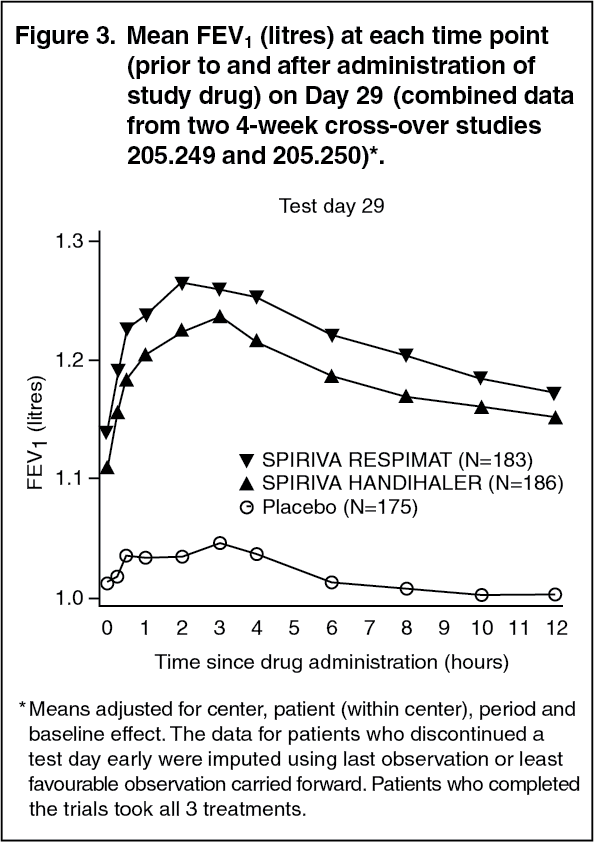 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA combined analysis of two randomised, placebo-controlled, crossover, clinical studies demonstrated that the bronchodilator response for SPIRIVA RESPIMAT (5 μg) was numerically higher compared to SPIRIVA HandiHaler (18 μg) inhalation powder after a 4-week treatment period.
Dyspnoea, Health-related Quality of Life, COPD Exacerbations in long-term 1 year studies: (a) Spiriva Respimat significantly improved dyspnoea (as evaluated using the Transition Dyspnoea Index) compared to placebo (mean improvement 1.05 units; 95% CI: 0.73 to 1.38 units, p<0.0001). An improvement was maintained throughout the treatment period.
(b) The improvement in mean total score of patient's evaluation of their Quality of Life (as measured using the St. George's Respiratory Questionnaire) between Spiriva Respimat versus placebo at the end of the two 1-year studies was 3.5 units (95% CI: 2.1 to 4.9, p<0.0001). A 4-unit decrease is considered clinically relevant.
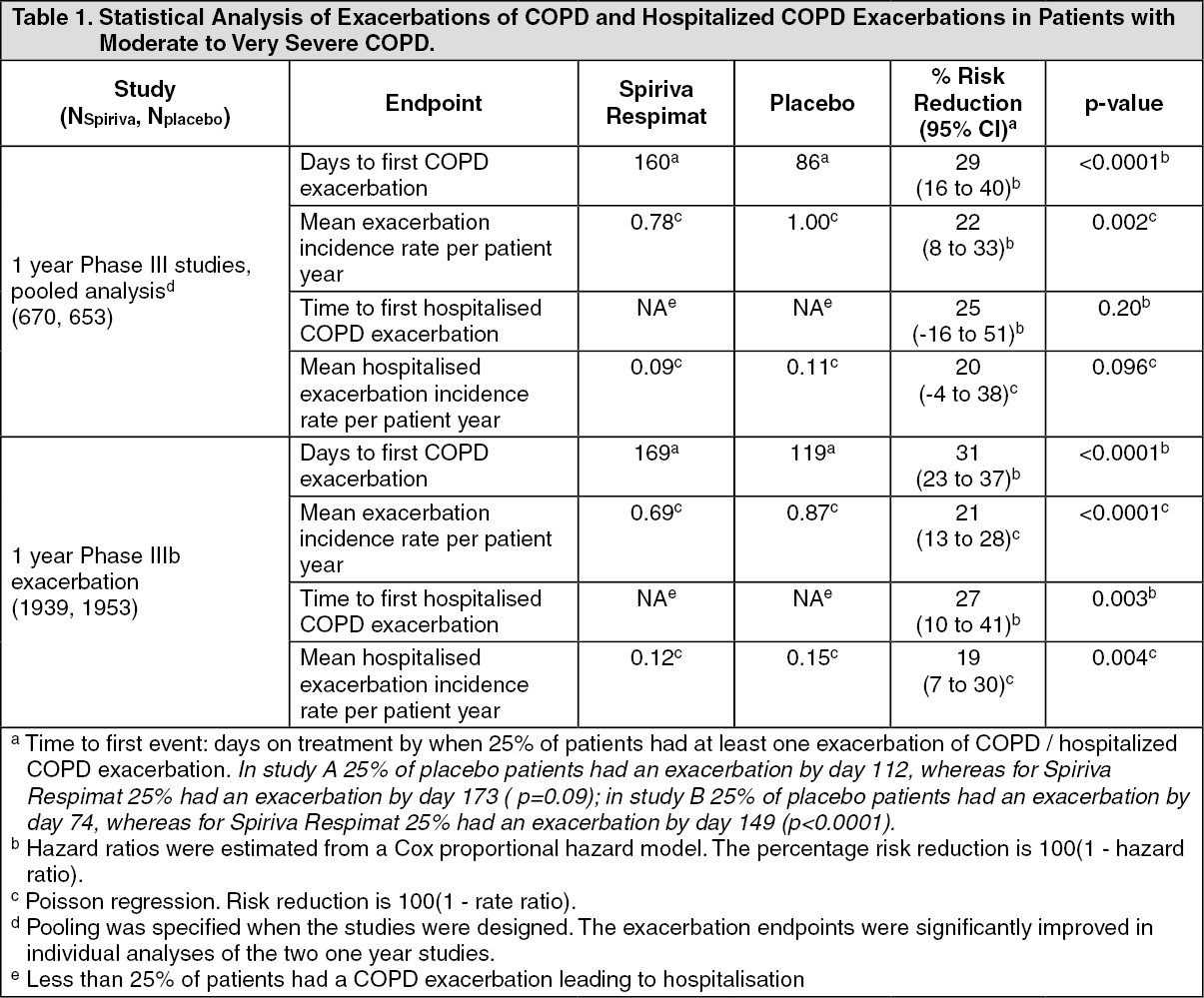
(c) COPD Exacerbations: In three one-year, randomised, double-blind, placebo-controlled clinical trials SPIRIVA RESPIMAT treatment resulted in a significantly reduced risk of a COPD exacerbation in comparison to placebo. Exacerbations of COPD were defined as "a complex of at least two respiratory events/symptoms with a duration of three days or more requiring a change in treatment (prescription of antibiotics and/or systemic corticosteroids and/or a significant change of the prescribed respiratory medication)". SPIRIVA RESPIMAT treatment resulted in a reduced risk of a hospitalisation due to a COPD exacerbation (significant in the appropriately powered large exacerbation trial).
The pooled analysis of two Phase III trials and separate analysis of an additional exacerbation trial is displayed in Table 1. All respiratory medications except anticholinergics and long-acting beta-agonists were allowed as concomitant treatment, i.e. rapidly acting beta-agonists, inhaled corticosteroids and xanthines. Long-acting beta-agonists were allowed in addition in the exacerbation trial. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLong-term tiotropium active-controlled study: A long term, large scale, randomised, double-blind, active-controlled study with a treatment period up to 3 years has been performed to compare the efficacy and safety of SPIRIVA RESPIMAT and SPIRIVA HANDIHALER (5,711 patients receiving SPIRIVA RESPIMAT 2.5 microgram [5 microgram medicinal dose]; 5,694 patients receiving SPIRIVA HANDIHALER). The primary endpoints were time to first COPD exacerbation, time to all-cause mortality and in a sub-study (906 patients) trough FEV1 (pre-dose).
The time to first COPD exacerbation was similar during the study with SPIRIVA RESPIMAT and SPIRIVA HANDIHALER (hazard ratio (SPIRIVA RESPIMAT/SPIRIVA HANDIHALER) 0.98 with a 95% CI of 0.93 to 1.03).
The median number of days to the first COPD exacerbation was 756 days for SPIRIVA RESPIMAT and 719 days for SPIRIVA HANDIHALER.
The bronchodilator effect of SPIRIVA RESPIMAT was sustained over 120 weeks, and was similar to SPIRIVA HANDIHALER. The mean difference in trough FEV1 for SPIRIVA RESPIMAT versus SPIRIVA HANDIHALER was -0.010 L (95% CI -0.038 to 0.018 mL).
All-cause mortality was similar during the study with SPIRIVA RESPIMAT and SPIRIVA HANDIHALER (hazard ratio [SPIRIVA RESPIMAT/SPIRIVA HANDIHALER] 0.96 with a 95% CI of 0.84 to 1.09).
Asthma: Adult patients: The clinical Phase III programme for persistent asthma included two 1-year, two 6-month and one 12-week, randomised, double-blind, placebo-controlled studies in a total of 3,476 asthma patients (1,128 receiving SPIRIVA RESPIMAT) on background treatment of at least ICS or ICS/LABA. The two 6-month studies were also active-controlled (salmeterol). All 5 studies included lung function measurements, assessments of symptoms including exacerbations, and health-related quality of life.
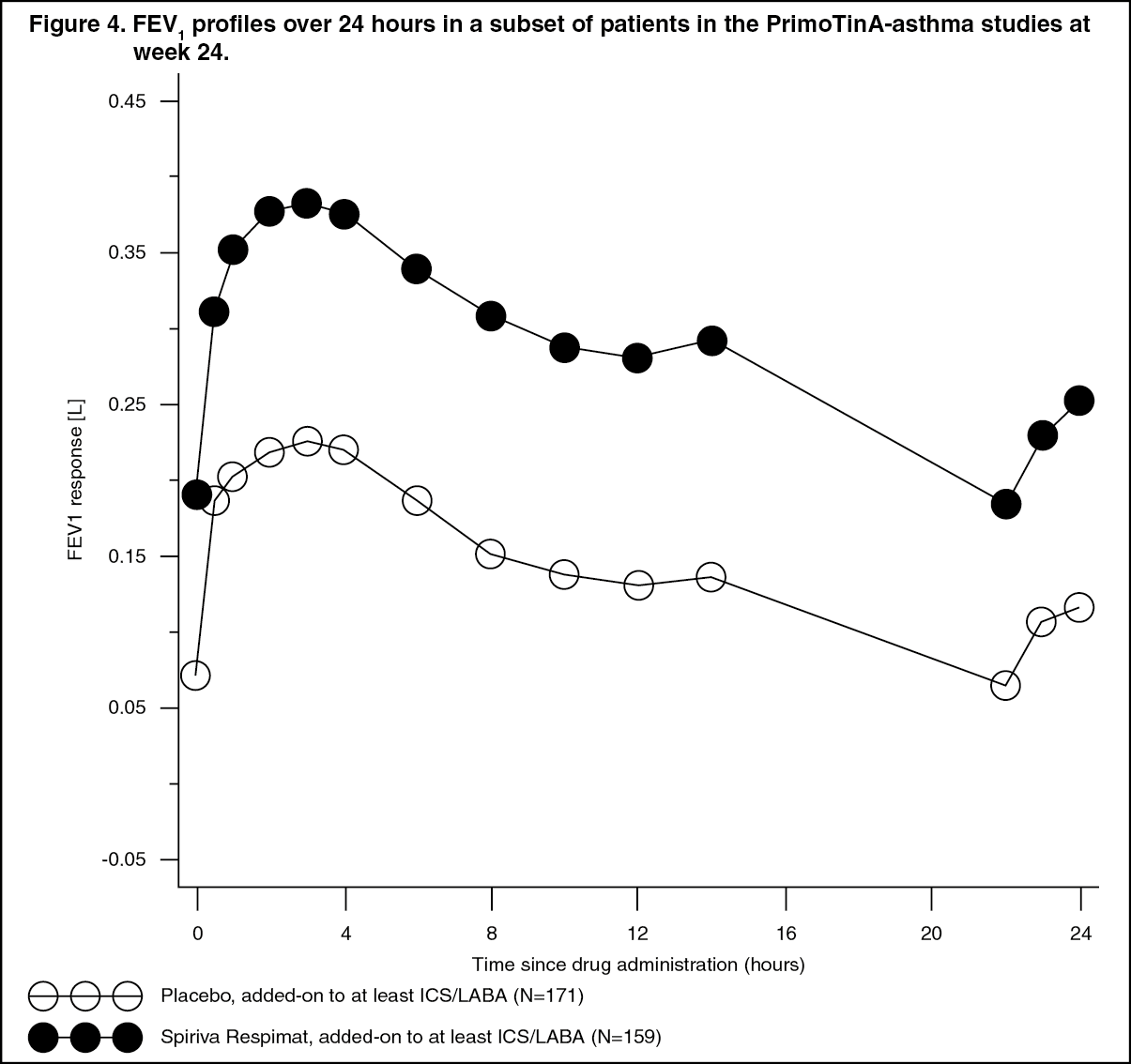
In the two 1-year PrimoTinA-asthma studies in patients who were symptomatic on maintenance treatment of at least high-dose ICS plus LABA, SPIRIVA RESPIMAT showed significant improvements in lung function over placebo when used as add-on to background treatment.
At week 24, mean improvements in peak and trough FEV1 were 0.110 litres (95% CI: 0.063 to 0.158 litres, p<0.0001) and 0.093 litres (95% CI: 0.050 to 0.137 litres, p<0.0001), respectively.
The improvement of lung function compared to placebo was maintained for 24 hours (Figure 4). (See Figure 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAt week 24, SPIRIVA RESPIMAT significantly improved morning and evening peak expiratory flow (PEF; mean improvement in the morning 23 L/min; 95% CI: 16 to 29 L/min, p< 0.0001; evening 26 L/min; 95% CI: 20 to 33 L/min, p<0.0001).
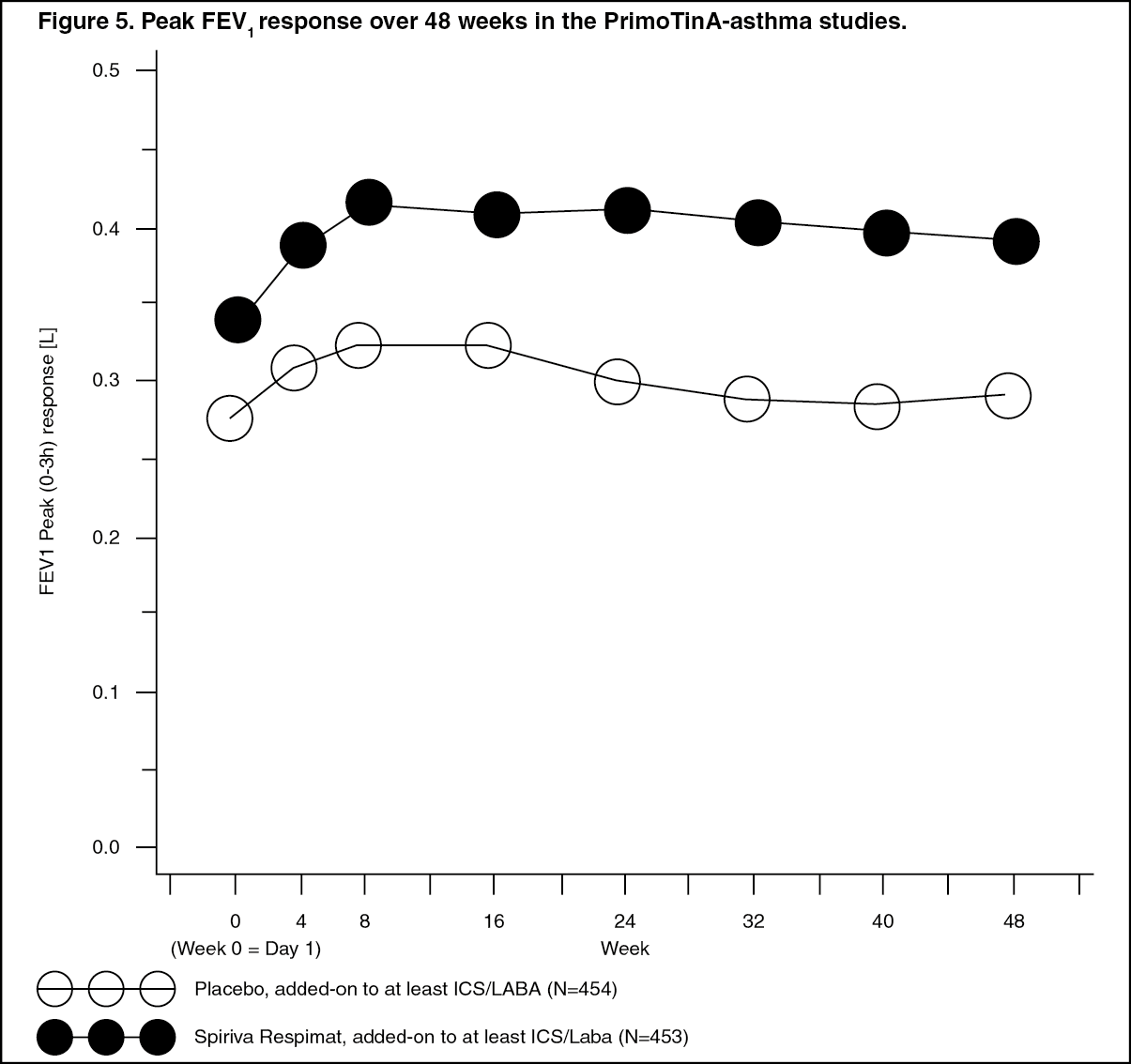
The bronchodilator effects of SPIRIVA RESPIMAT were maintained throughout the 1 year period of administration with no evidence of tachyphylaxis or tolerance. (See Figure 5.)
 Click on icon to see table/diagram/image
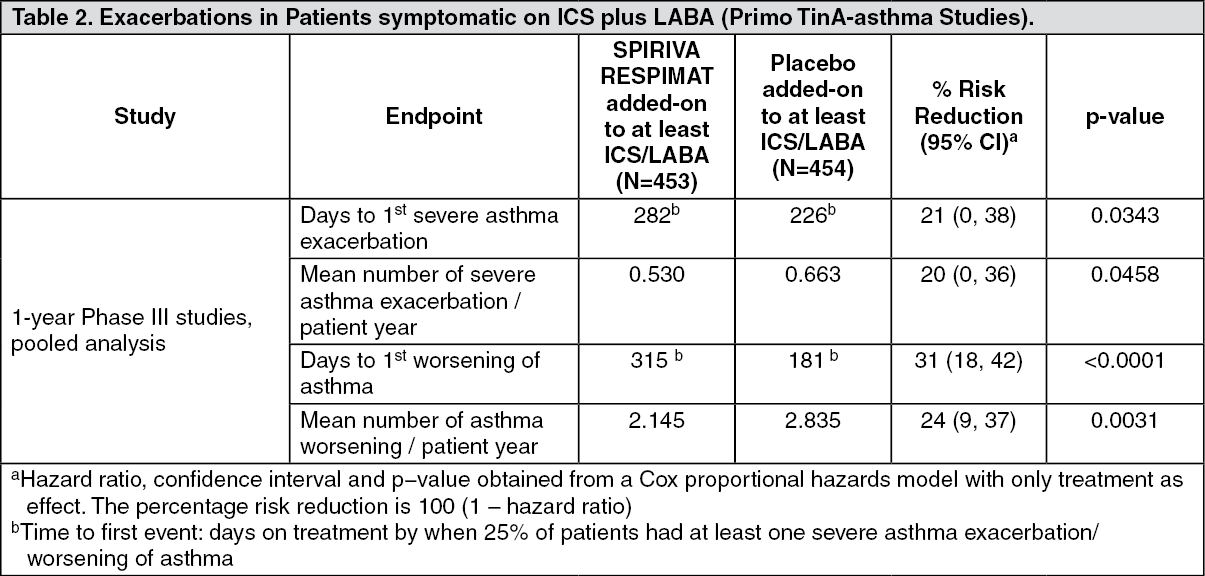
Click on icon to see table/diagram/imageSPIRIVA RESPIMAT significantly reduced the risk of severe asthma exacerbations (see Table 2 and Figure 6).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image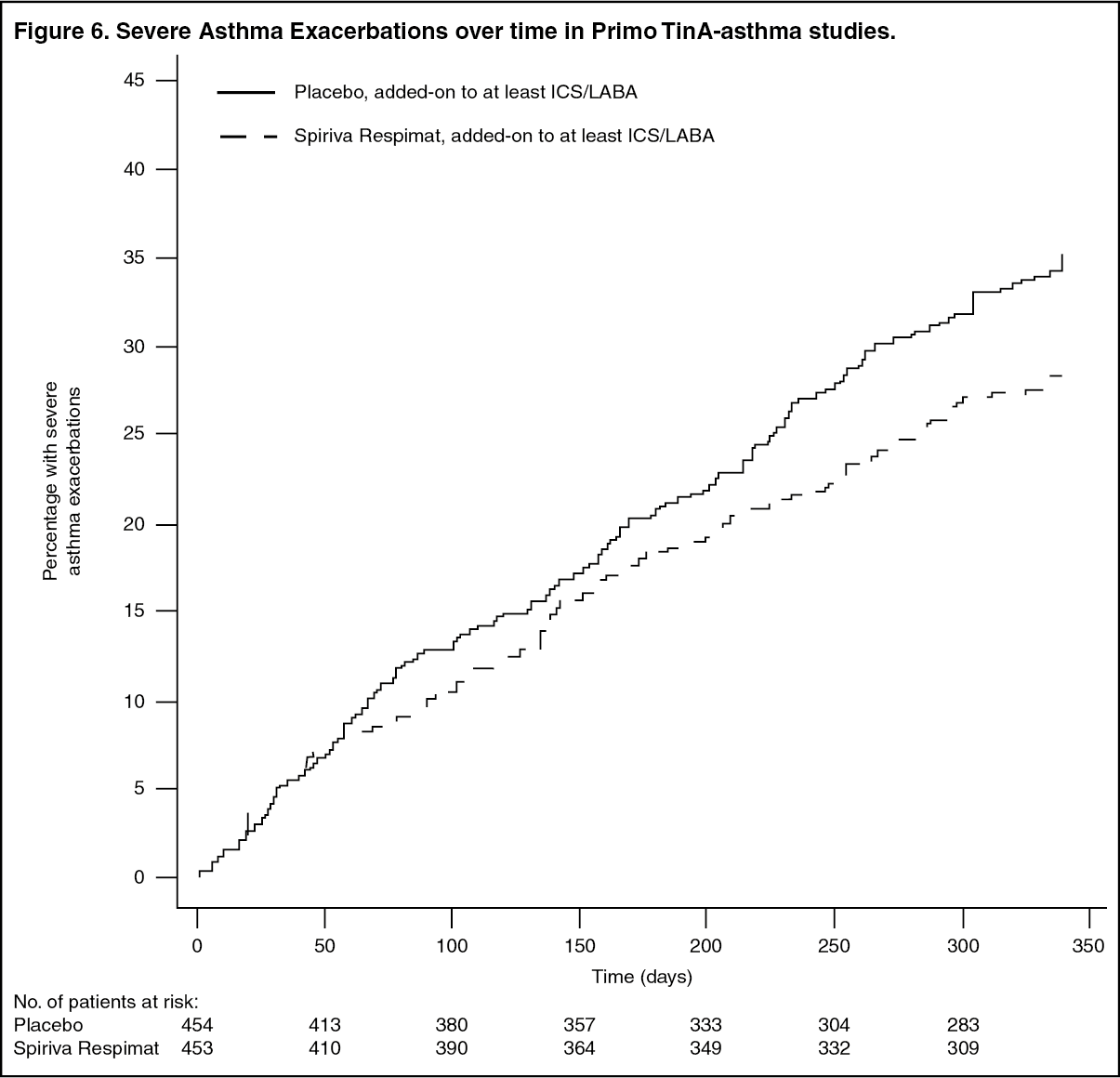 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe Asthma Control Questionnaire (ACQ) responder rates defined as percentage of patients improving by at least 0.5 points, were significantly higher with SPIRIVA RESPIMAT (53.9% versus 46.9%; p=0.0427).
The Asthma Quality of Life Questionnaire (AQLQ(S)) mean scores for SPIRIVA RESPIMAT improved significantly over placebo at week 24.
In the two 6-month MezzoTinA-asthma studies in patients who were symptomatic on maintenance treatment of medium-dose ICS, SPIRIVA RESPIMAT showed significant improvements in lung function over placebo when used as add-on to background treatment.
At week 24, mean improvements in peak and trough FEV1 were 0.185 litres (95% CI: 0.146 to 0.223 litres, p<0.0001) and 0.146 litres (0.105 to 0.188 litres, p<0.0001), respectively. The peak and trough FEV1 values for salmeterol were 0.196 litres (95% CI: 0.158 to 0.234 litres) and 0.114 litres (95% CI: 0.073 to 0.155 litres), respectively.
SPIRIVA RESPIMAT significantly improved morning and evening PEF (morning 24 L/min; 95% CI: 18 to 31 L/min, p< 0.0001; evening 23 L/min; 95% CI: 17 to 30 L/min, p<0.0001). The morning and evening PEF for salmeterol compared to placebo were 25 L/min (95% CI: 19 to 31 L/min) and 21 L/min (95% CI: 15 to 27 L/min), respectively.
Patients who took SPIRIVA RESPIMAT had a significantly higher ACQ responder rate at week 24 compared to patients taking placebo (Table 3). (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the 12 week GraziaTinA-asthma study in patients who were symptomatic on maintenance treatment with low dose ICS, SPIRIVA RESPIMAT showed significant improvements in lung function over placebo when used as add-on to background treatment. At 12 weeks, the mean improvements in peak and trough FEV1 were 0.128 litres (95% CI: 0.057 to 0.199 litres, p<0.0005) and 0.122 litres (95% CI: 0.049 to 0.194 litres, p<0.0010), respectively.
Paediatric Patients: The clinical Phase III program for persistent asthma in paediatric patients (1-17 years) included: Adolescents (12-17 years): one 1-year and one 12-week randomised, double-blind, placebo-controlled studies in a total of 789 asthma patients (264 receiving SPIRIVA RESPIMAT).
Children (6-11 years): one 1-year and one 12-week randomised, double-blind, placebo-controlled studies in a total of 801 asthma patients (265 receiving SPIRIVA RESPIMAT).
Children (1-5 years): one 12-week randomised, double-blind, placebo-controlled study in a total of 101 asthma patients (31 receiving SPIRIVA RESPIMAT).
In all these studies, patients were on background treatment of at least ICS.
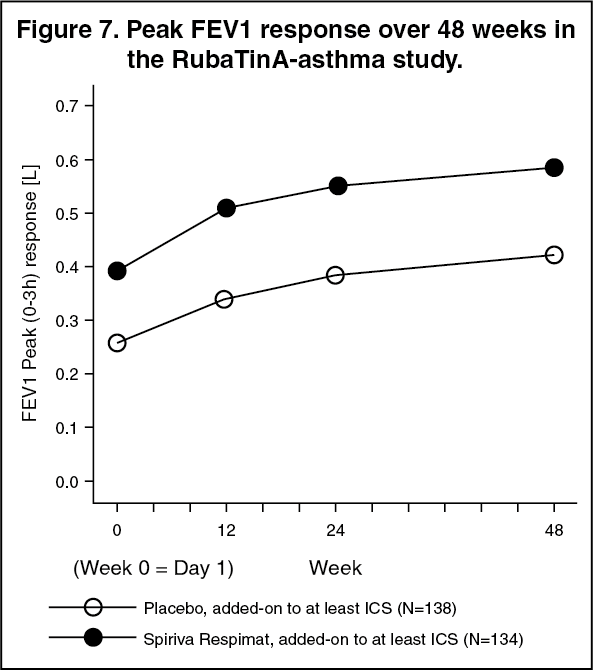
Adolescents (12-17 years): In the 1-year RubaTinA-asthma study in patients who were symptomatic on maintenance treatment of at least medium-dose ICS, SPIRIVA RESPIMAT showed significant improvements in lung function over placebo when used as add-on to background treatment.
At week 24, mean improvements in peak and trough FEV1 were 0.174 litres (95% CI: 0.076 to 0.272 litres, p=0.0005) and 0.117 litres (95% CI: 0.010 to 0.223 litres, p=0.0320), respectively.
At week 24, SPIRIVA RESPIMAT significantly improved morning and evening PEF (morning 15.8 L/min; 95% CI: 2.3, 29.3 L/min, p=0.0214; evening 16.7 L/min; 95% CI: 3.4, 30.0 L/min, p=0.0137).
The bronchodilator effects of SPIRIVA RESPIMAT were maintained throughout the 1 year period of administration with no evidence of tachyphylaxis (Figure 7). (See Figure 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the 12-week PensieTinA-asthma study in patients who were symptomatic on maintenance treatment of at least medium dose ICS in combination with 1 or more controller medication, SPIRIVA RESPIMAT showed improvements in lung function over placebo when used as add-on to background treatment, however, the differences in peak and trough FEV1 were not statistically significant.
At week 12, mean improvements in peak and trough FEV1 were 0.090 litres (95% CI: -0.019 to 0.198 litres, p=0.1039) and 0.054 litres (95% CI: -0.061 to 0.168 litres, p=0.3605), respectively.
At week 12, SPIRIVA RESPIMAT significantly improved morning and evening PEF (morning 17.4 L/min; 95% CI: 5.1 to 29.6 L/min; evening 17.6 L/min; 95% CI: 5.9 to 29.6 L/min).
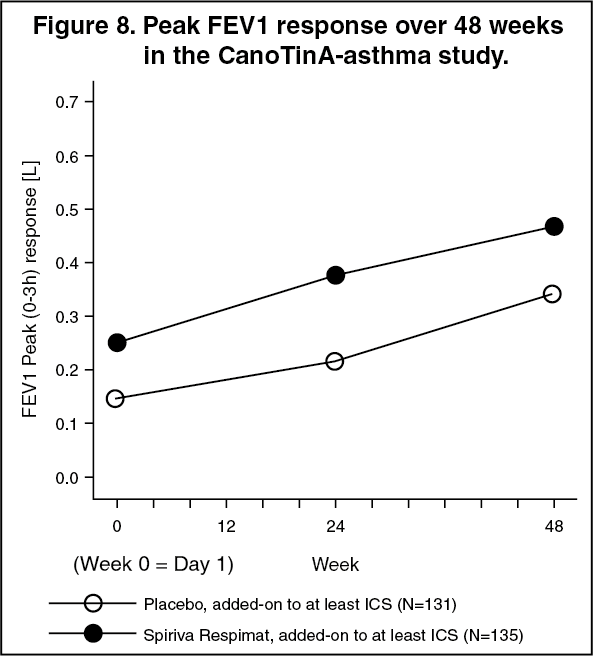
Children (6-11 years): In the 1-year CanoTinA-asthma study in patients who were symptomatic on maintenance treatment of at least medium-dose ICS, SPIRIVA RESPIMAT showed significant improvements in lung function and asthma control over placebo when used as add-on to background treatment.
At week 24, mean improvements in peak and trough FEV1 were 0.164 litres (95% CI: 0.103 to 0.225 litres, p<0.0001) and 0.118 litres (95% CI: 0.048 to 0.188 litres, p=0.0010), respectively.
The bronchodilator effects of SPIRIVA RESPIMAT were maintained throughout the 1 year period of administration with no evidence of tachyphylaxis (Figure 8). (See Figure 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the 12-week VivaTinA-asthma study in patients who were symptomatic on maintenance treatment of at least medium dose ICS in combination with 1 or more controller medication, SPIRIVA RESPIMAT showed significant improvements in lung function over placebo when used as add-on to background treatment.
At week 12, mean improvements in peak and trough FEV1 were 0.139 litres (95% CI: 0.075 to 0.203 litres, p<0.0001) and 0.087 litres (95% CI: 0.019 to 0.154 litres, p=0.0117), respectively.
Pharmacokinetics: General Introduction: Tiotropium bromide is a non-chiral quaternary ammonium compound and is sparingly soluble in water. Tiotropium bromide is available as inhalation solution administered by the Respimat inhaler. Approximately 40% of the inhaled dose is deposited in the lungs, the target organ, the remaining amount being deposited in the gastrointestinal tract. Some of the pharmacokinetic data described as follows were obtained with higher doses than recommended for therapy.
General Characteristics of the Active Substance after Administration of the Medicinal Product: Absorption: Following inhalation by young healthy volunteers, urinary excretion data suggest that approximately 33% of the inhaled dose reaches the systemic circulation. Oral solutions of tiotropium bromide have an absolute bioavailability of 2-3%. Food is not expected to influence the absorption of this quaternary ammonium compound.
Maximum tiotropium plasma concentrations were observed 5-7 minutes after inhalation. At steady state, peak tiotropium plasma concentrations of 10.5 pg/ml were achieved in COPD patients and decreased rapidly in a multi-compartmental manner. Steady state trough plasma concentrations were 1.60 pg/ml.
At steady-state tiotropium peak plasma concentration of 5.15 pg/mL was attained 5 minutes after the administration of the same dose to patients with asthma.
Distribution: The drug has a plasma protein binding of 72% and shows a volume of distribution of 32 L/kg.
Local concentrations in the lung are not known, but the mode of administration suggests substantially higher concentrations in the lung. Studies in rats have shown that tiotropium does not penetrate the blood-brain barrier to any relevant extent.
Biotransformation: The extent of biotransformation is small. This is evident from a urinary excretion of 74% of unchanged substance after an intravenous dose to young healthy volunteers. The ester tiotropium bromide is nonenzymatically cleaved to the alcohol (N-methylscopine) and acid compound (dithienylglycolic acid) that are inactive on muscarinic receptors.
In-vitro experiments with human liver microsomes and human hepatocytes suggest that some further drug (<20% of dose after intravenous administration) is metabolised by cytochrome P450 (CYP) dependent oxidation and subsequent glutathione conjugation to a variety of Phase II-metabolites.
In vitro studies in liver microsomes reveal that the enzymatic pathway can be inhibited by the CYP 2D6 (and 3A4) inhibitors, quinidine, ketoconazole and gestodene. Thus CYP 2D6 and 3A4 are involved in metabolic pathway that is responsible for the elimination of a smaller part of the dose. Tiotropium bromide even in supra-therapeutic concentrations does not inhibit CYP 1A1, 1A2, 2B6, 2C9, 2C19, 2D6, 2E1 or 3A in human liver microsomes.
Elimination: The effective half-life of tiotropium ranges between 27 to 45h following inhalation by COPD patients.
The effective half-life was 34 hours in patients with asthma.
Total clearance was 880 mL/min after an intravenous dose in young healthy volunteers. Intravenously administered tiotropium bromide is mainly excreted unchanged in urine (74%). After inhalation of the solution by COPD patients urinary excretion is 18.6 % (0.93 μg) of the dose, the remainder being mainly non-absorbed drug in gut that is eliminated via the faeces.
In patients with asthma, 11.9% (0.595 μg) of the dose is excreted unchanged in the urine over 24 hours post dose at steady state.
The renal clearance of tiotropium exceeds the creatinine clearance, indicating secretion into the urine. After chronic once daily inhalation by COPD patients, pharmacokinetic steady-state was reached by day 7 with no accumulation thereafter.
Linearity/Nonlinearity: Tiotropium demonstrates linear pharmacokinetics in the therapeutic range independent of the formulation.
Characteristics in Patients: Geriatric Patients: As expected for all predominantly renally excreted drugs, advancing age was associated with a decrease of tiotropium renal clearance from 347 mL/min in COPD patients <65 years to 275 mL/min in COPD patients ≥65 years. This did not result in a corresponding increase in AUC0-6,ss or Cmax,ss values.
Exposure to tiotropium was not found to differ with age in patients with asthma.
Paediatric Patients: Asthma: The peak and total (AUC and urinary excretion) exposure to tiotropium is comparable between patients with asthma who were 6 - 11 years old, 12 - 17 years old and ≥18 years old. Based on urinary excretion, the total exposure to tiotropium in patients 1 to 5 years of age was 52 to 60% lower than in other older age groups. The total exposure data when adjusted for body surface area were found to be comparable in all age groups. Spiriva Respimat was administered with a valved holding chamber with face mask in patients 1 to 5 years of age.
COPD: There were no paediatric patients in the COPD programme (see Dosage & Administration).
Renally Impaired Patients: Following once daily inhaled administration of tiotropium to steady-state in COPD patients with mild renal impairment (CLCR 50-80 mL/min) resulted in slightly higher AUC0-6,ss (between 1.8 to 30% higher) and similar Cmax,ss compared to patients with normal renal function (CLCR >80 mL/min). In COPD patients with moderate to severe renal impairment (CLCR <50 mL/min) the intravenous administration of tiotropium bromide resulted in doubling of the total exposure (82% higher AUC0-4h) and 52% higher Cmax) compared to COPD patients with normal renal function, which was confirmed by plasma concentrations after dry powder inhalation.
In asthma patients with mild renal impairment (CLCR 50-80 mL/min) inhaled tiotropium did not result in relevant increases in exposure compared to patients with normal renal function.
Hepatically Impaired Patients: Liver insufficiency is not expected to have any relevant influence on tiotropium bromide pharmacokinetics. Tiotropium bromide is predominantly cleared by renal elimination (74% in young healthy volunteers) and simple non-enzymatic ester cleavage to pharmacologically inactive products.
Pharmacokinetic/Pharmacodynamic Relationship(s): There is no direct relationship between pharmacokinetics and pharmacodynamics.
Toxicology: Preclinical safety data: Many effects observed in conventional studies of safety pharmacology, repeat-dose toxicity, and reproductive toxicity could be explained by the anticholinergic properties of tiotropium bromide. Typically in animals reduced food consumption, inhibited body weight gain, dry mouth and nose, reduced lacrimation and salivation, mydriasis and increased heart rate were observed. Other relevant effects noted in repeated dose toxicity studies were: mild irritancy of the respiratory tract in rats and mice evinced by rhinitis and epithelial changes of the nasal cavity and larynx, and prostatitis along with proteinaceous deposits and lithiasis in the bladder in rats.
In juvenile rats exposed from postnatal day 7 to sexual maturity, the same direct and indirect pharmacological changes were observed as in the repeat-dose toxicity studies as well as rhinitis. No systemic toxicity was noted and no toxicologically relevant effects on key developmental parameters, tracheal or key organ development were seen.
Harmful effects with respect to pregnancy, embryonal/foetal development, parturition or postnatal development could only be demonstrated at maternally toxic dose levels. Tiotropium bromide was not teratogenic in rats or rabbits. In a general reproduction and fertility study in rats, there was no indication of any adverse effect on fertility or mating performance of either treated parents or their offspring at any dosage.
The respiratory (irritation) and urogenital (prostatitis) changes and reproductive toxicity was observed at local or systemic exposures more than five-fold the therapeutic exposure. Studies on genotoxicity and carcinogenic potential revealed no special hazard for humans.